Ultrasound appears to be an effective and safe diagnostic workup modality when it comes to evaluating masses identified on screening digital breast tomosynthesis (DBT), according to research published in the European Journal of Radiology (EJR).
The findings suggest that, at least in the case of breast masses, it may not be necessary for women to undergo both digital mammography and ultrasound after screening DBT -- which has the benefit of reducing radiation exposure, wrote a group led by Dr. Jessica Porembka of the University of Texas Southwestern Medical Center in Dallas.
"DBT has been shown to be superior to conventional views in the diagnostic setting ... [and] women who already underwent screening DBT may be receiving unnecessary digital mammography prior to ultrasound imaging," the group wrote in an EJR article posted on August 5. "This potentially adds unnecessary complexity, cost, and radiation exposure, as well as prolonged diagnostic workup times without adding significant value."
Screening DBT reduces recalls compared with digital mammography alone, but still, sometimes follow-up is needed. Porembka and colleagues investigated whether in some of these cases --perhaps by type of lesion found on DBT -- women could undergo ultrasound alone rather than also having additional mammography.
The study included 266 noncalcified lesions in 247 women detected on screening DBT between January 2014 and December 2016. The lesions ranged from architectural distortions and asymmetries to focal asymmetries and masses. The investigators assessed the number and type of lesions that underwent diagnostic follow-up only with ultrasound.
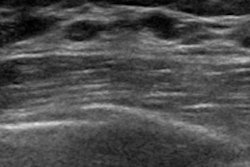
The researchers found that ultrasound alone was used in 69% of workups of recalled masses, and that the odds of masses being worked up with ultrasound alone was eight times that of the odds of digital mammography and ultrasound being used. The authors also found that "ultrasound alone in the diagnostic evaluation of a mass seen on screening DBT had a higher yield of true lesions than masses worked up with digital mammography/ultrasound," confirming that "masses seen on screening DBT can be adequately evaluated with ultrasound alone."
However, ultrasound alone did less well with architectural distortions and focal asymmetries, with a detection rate of 44% and 25%, respectively, Porembka and colleagues cautioned.
"Our findings suggest that a combination of both [digital mammography and ultrasound] was preferred by radiologists in the work up of architectural distortions given the differential diagnosis of radial scar versus malignancy," the team noted. "For focal asymmetries, 68% were evaluated with digital mammography/ultrasound, while only 25% were evaluated with ultrasound alone, indicating that a combination of digital mammography/ultrasound is likely warranted in the work up of focal asymmetry on DBT."
In any case, the study results are good news for women undergoing diagnostic follow-up for masses found on screening DBT, according to the researchers.
"The implication of our findings is that we can save women unnecessary radiation and unnecessary cost of digital mammography by utilizing ultrasound alone in the evaluation of recalled masses," they concluded.