Clinical and ultrasound features improve diagnostic accuracy for detecting endometrial malignancy, suggest findings published April 21 in the Journal of Radiation Research and Applied Sciences.
Researchers led by Xiu Yun Dong from the Jinan Maternal and Child Health Hospital Affiliated to Shandong First Medical University in China found that incorporating these features into their risk stratification model led to marked improvement in finding endometrial malignancy.
“This approach provides a practical and personalized method for identifying high-risk postmenopausal women, helping to target interventions and reduce unnecessary procedures,” Dong and co-authors wrote.
While most cases of asymptomatic endometrial thickening are benign, women are still at risk of having an underlying malignancy. However, it remains a challenge to determine which women need further testing.
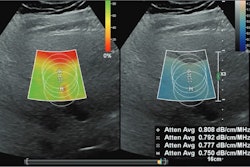
Dong and colleagues created a multivariable risk stratification model that used clinical features and features from transvaginal ultrasound (TVUS) images. They sought to find out whether their model could detect endometrial malignancy and precursor lesions in postmenopausal women with asymptomatic endometrial thickening.
The study included retrospective data from 587 women with asymptomatic endometrial thickening identified during routine TVUS exams. The team divided the women into a positive group (n = 221 women with malignant or precursor lesions) and a negative group (n = 366 women with benign lesions), based on histopathological results. For the model, the researchers collected data on endometrial thickness, ultrasound features, and clinical risk factors such as age, body mass index (BMI), and diabetes status.
The positive group experienced a significantly higher average endometrial thickness compared with the negative group (14.2 mm vs. 10.1 mm, p < 0.001).
Ultrasound features like irregular endometrial borders and heterogeneous echotexture were more commonly seen in the positive group (34.5 % vs. 7.5 %, p < 0.001).
The researchers also highlighted the following independent predictors of malignancy on multivariable analysis: endometrial thickness (odds ratio [OR], 2.94; p < 0.001), ultrasound abnormalities (OR, 4.12; p < 0.001), diabetes (OR, 1.98; p < 0.001), and BMI ≥ 30 kg/m2 (OR, 1.82; p = 0.009).
Finally, the predictive model that combined these features achieved an area under the curve of 0.81 (with 1 as reference).
The study authors wrote that including clinical and imaging factors allows the risk model to provide “a more comprehensive understanding” of the relationship between metabolic health and endometrial pathology.
“Including these features in risk stratification models can help clinicians prioritize patients for invasive diagnostic procedures, such as hysteroscopy or biopsy,” they wrote. “Moreover, incorporating clinical risk factors into the model aligns with the principles of personalized medicine, enabling more tailored care.”
The authors also called for future studies to focus on validating this model in diverse populations and exploring emerging imaging technologies to further improve early detection and risk stratification.
The full study can be found here.