The term "angiodysplasia" describes a wide range of vascular malformations, both congenital and acquired. Classifying the lesions accurately and defining the extent of disease are essential steps for optimal management and treatment. However, assessment is a difficult process that usually requires a combination of imaging modalities.
At the 2002 European Congress of Radiology in Vienna, Dr. Christoph Herborn from the radiology department of University Hospital in Essen, Germany, discussed MRI and MRA imaging as promising techniques that could potentially replace conventional angiography and ultrasound.
"The congenital forms of angiodysplasia are either the typical arteriovenous malformations, or may occur within systemic disorders such as Klippel-Trénaunay syndrome," he said. "The acquired forms can easily be due to traumatic events, or iatrogenic due to postinterventional events. They can be contained in the subcutaneous tissue as well as the mucous tissue. They often have multiple manifestations in the breast, with multiple microshunts or fistulas which might impair the function of peripheral extremities."
Beyond the accurate assessment of disease extent, evaluation requires distinguishing among several different types of lesions -- for example, differentiating capillary or cavernous hemangiomas from arteriovenous angiomas or purely venous hemangiomas, Herborn said.
But venography and plethysmography are invasive, and sonography can be unreliable. So the researchers sought to assess the characterization of angiodysplasia with MRI and MRA compared to Doppler ultrasound and conventional angiography.
Herborn and colleagues, Dr. Mathias Goyen, Dr. Knut Kroeger, Dr. Thomas Luenstein, Dr. Jörg Debatin, and Dr. Stefan Ruehm, examined 14 patients, including 9 men and 5 women aged 10-64 (mean age 47.3). All patients had known peripheral arteriovenous malformations according to a standard of reference that included digital subtraction angiography (DSA) and/or duplex Doppler sonography, as well as clinical findings.
The images were acquired on a 1.5-tesla Magnetom Sonata scanner (Siemens Medical Solutions, Erlangen, Germany), using dedicated extremity and body-array surface coils whenever possible.
"We used a T1-weighted 2-D FLASH (fast low-angle shot) sequence in an axial acquisition; T2-weighted spin echo, also in an axial acquisition; then a STIR (short tau inversion recovery) sequence with both axial and coronal acquisitions; and finally a dynamic 3-D FLASH sequence with coronal acquisition following the injection of a body weight-adjusted dose of gadolinium contrast," Herborn said.
 |
Radiologists interpreted the images in an effort to detect and localize the lesions -- especially the extent and involvement of neighboring structures -- and classify them.
All of the MR examinations were of diagnostic quality. Together MRI/MRA detected a total of 11 arteriovenous angiomas; and 7 hemangiomas, including 4 angiomas with microshunts, 2 arteriovenous fistulas, both congenital, and one patient with Klippel-Trénaunay syndrome. All manifestations of the lesions were subcutaneous, but 6 of the patients also had bone and muscle involvement, Herborn said.
 |
"(Above) is a male patient with AVM, which looks like some kind of vericosis," he said. However, the cross-section shows the (AVM) defect, which is underestimated on the T1- weighted images, clearer in the T2-weighted images, and even better in the STIR images, which show involvement of the musculature and tibia bone.
"The contrast-enhanced images provide some comparable information for the muscular and bone manifestation of the disease," Herborn said. "The coronal STIR images show (AVM) presence inside the tibia, as well as in the subcutaneous and intramuscular tissue. The arterial phase of the contrast-enhanced sequence just covers the structures like bones and muscles, and therefore nicely shows the small vessels feeding a microshunt."
 |
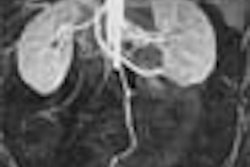
| Above and below: 43-year-old male with Klippel-Trénaunay syndrome. Below, contrast-enhanced MRA images clearly depict arterial vessels, cross-sectional images enable accurate assessment of lesion extent, and STIR images accurately depict the extent of disease. Images and graphics courtesy of Dr. Christoph Herborn. |
 |
Overall, the STIR sequence was helpful for determining the extent of vascular malformation, which MRA alone tended to underestimate, Herborn said. Dynamic MRA was needed to accurately classify the lesion type. Compared to the reference standard (DSA and/or Doppler US), the sensitivity of MRA/MRI imaging for classifying lesion type was 100%, with specificity of 91%.
The results were well correlated with conventional angiography (N=11) and Duplex ultrasound (N=16), Herborn said.
 |
"From this data one can conclude that MRI and MR angiography permit concomitant assessment of angiodysplastic lesions, and multiphase (contrast-enhanced) 3-D GRE (gradient-recalled echo) provides functional information, (while) the true information about the extent of the lesion lies in the cross-sectional images," he said.
"The STIR and T2-weighted images were really helpful for determination of lesion extent. Although these results are pretty promising, one should keep in mind that the exact noninvasive classification of angiodysplasia (type) remains challenging, and still depends on a combination of different radiological modalities."
By Eric BarnesAuntMinnie.com staff writer
April 25, 2002
Copyright © 2002 AuntMinnie.com