Sarcoidosis is a disease of unknown origin that affects fewer than 1 in 5,000 people. It can be temporary or permanent, invisible or debilitating, and is characterized by the formation of inflamed tissue in virtually any body or organ system. Anti-inflammatory drugs such as prednisone have proven effective in inhibiting tissue growth, while gentler approaches such as the low-inflammation diet have been used in milder cases.
Where sarcoidosis gets grim is in the heart, wherein the patient's first symptom is often sudden death. At the 2002 European Congress of Radiology in Vienna, Dr. Olivier Vignaux from Hôpital Cochin and the University of Paris in France discussed his group's study of cardiac sarcoidosis. The group concluded that more frequent monitoring with MRI could save lives.
"The pathological features of cardiac sarcoidosis include patchy infiltration of the myocardium with edema, and fibrosis leading to postinflammatory scarring," Vignaux said. "Cardiac involvement is symptomatic in only 5% of patients. Most patients with myocardial sarcoidosis will remain asymptomatic, but sudden death accounts for up to 65% of the fatalities. Early initiation of steroids enables an improvement in left ventricular function and prevents malignant arrhythmias."
Imaging modalities such as echocardiography and thallium scans suffer from either low specificity or sensitivity, he said, and endomyocardial biopsy may be negative due to the patchy distribution of the lesions. MRI experience has been limited to a few case studies.
Experience in cardiac MRI has so far been limited to several case reports, Vignaux said, while a recent study by Dr. Toshio Shimata and colleagues emphasized the usefulness of gadolinium or DPTA-enhanced MRI imaging (American Journal of Medicine, May 2001, Vol 110:7, pp. 520-527).
"The purpose of our study was to prospectively assess cardiac MR features in ongoing sarcoidosis," Vignaux said, "and to evaluate the clinical and MR follow-up of patients with cardiac MR abnormalities so as to clarify the clinical significance of these abnormalties, and thereby assess the role of cardiac MRI in the management of such patients."
The study examined 45 patients (27 male, 18 female, mean age of 38.8 ± 12.2) with histologically proven sarcoidosis (including 9 with chest involvement, and 36 with multiple organ involvement). Patients with heart disease were excluded following cardiac assessment that included examination with CT, ECG, 24-hour Holter monitoring, and echocardiography. In addition, coronary angiography was performed in patients over 40, or with suspected cardiac disease. Six-month follow-up (all patients) and 12-month follow-up (12/45 patients) included physical exam, ECG, and MRI.
T1-weighted, gadolinium-DTPA-enhanced spin-echo and segmented gradient-echo MR images, as well as T2-weighted single-shot fast spin-echo (SSFSE), and short tau inversion recovery fast-spin-echo (STIR FSE) images were acquired of the heart. A 1.5-tesla Signa scanner (GE Medical Systems, Waukesha, WI) was used to acquire axial, left-ventricular long-axis, left-ventricular short-axis, and four-chamber views for each patient, Vignaux said.
The images were analyzed by two radiologists who were unaware of the clinical findings. They assigned scores in 6 myocardial areas including the right ventricle (RV), septal, anterior, lateral, inferior, and posterior walls based on a qualitative evaluation of signal intensity. Zero was normal, indicating medium homogeneous signal intensity; +1 designated increased signal intensity higher than myocardial wall; and -1 was a hypointense area with signal intensity lower than normal myocardial wall.
Six patients presented with clinical evidence of cardiac involvement, which corresponded to MR abnormalities in all cases, he said. Thirty-nine patients were cardiac-asymptomatic; of these 13 had normal MRI results, and 7 had early-stage chest involvement (either stage I or Lofgren syndrome).
In all, MRI revealed cardiac abnormalities in 26 of 39 patients. Nine of the 26 had focal myocardial thickening. Among the T2-weighted patient images, 27 had focal intramyocardial increased signal, which was seen in only 21 of the gadolinium-enhanced T1-weighted images.
Cardiac involvement comprised three major patterns in MR, including:
- Septal nodular pattern depicted as increased signal intensity on both T2-weighted and gadolinium-DPTA-enhanced T1-weighted images.
- Inflammatory stage pattern showing increased signal intensity on both T2 and gadolinium-DPTA-enhanced T1-weighted images.
- Pattern suggesting postinflammatory scarring, with increased signal intensity visible on T2-weighted images.
 |
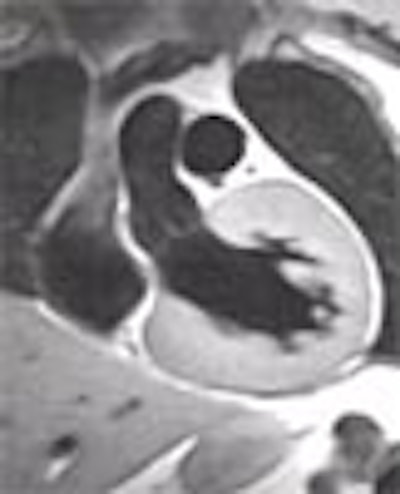
| In (Pattern B) inflammatory stage with edema shown above, increased signal intensity suggests inflammation in both T2-weighted MR images (left and center), while myocardial thickening can be seen using all three protocols. Graphics and images courtesy of Dr. Olivier Vignaux. |
MR regression or improvement was recorded after steroidal therapy in all patients. At 12-month follow-up analysis, disease activity was scored on the basis of physical exam, high-resolution chest CT, and visceral involvement including regression, improvement, stability, or worsening, Vignaux said. The initial MR score was then compared with the 12-month follow-up score, per the chart below.
 |
"Regarding the follow-up chart (above), a worsening of MR features was correlated with the worsening of sarcoidosis in two cases," Vignaux said. "It was even predictive of symptomatic cardiac involvement in one case during follow-up."
Vignaux concluded that MRI highlights the occurrence of subclincial sarcoidosis in patients with ongoing multiple system sarcoidosis, and demonstrates that cardiac MR features were correlated with clinical features in the follow-up study.
"Further studies are required to confirm the clinical significance," he said, "but we believe that MR imaging should be used more widely to investigate and follow up patients with ongoing sarcoidosis in order to detect early cardiac involvement, (whose) first manifestation is sudden death in as many as 65% of patients."
By Eric BarnesAuntMinnie.com staff writer
April 1, 2002
Copyright © 2002 AuntMinnie.com