Caution is in order when using low-dose CT (LDCT) protocols with computer-aided-detection (CAD) systems for diagnosing small lung nodules in children, according to a study published October 9 in the American Journal of Roentgenology (AJR).
A group led by Russell Hardie, PhD, of the University of Dayton in Ohio found that two lung-nodule CAD systems showed lower sensitivity on LDCT compared with standard-dose pediatric CT scans and that this reduced detection at low dose was more prominent for nodules smaller than 5 mm.
"Two lung-nodule CAD systems demonstrated decreased sensitivity on low-dose versus standard-dose pediatric CT scans performed in the same patients," Hardie said in a statement released by the AJR. "The reduced detection at low dose was overall more pronounced for nodules measuring less than 5 mm."
Chest CT is a common exam for children to diagnose and monitor lung disease, but exposing children to radiation is always a concern. LDCT has been used to mitigate this exposure, but its efficacy for the indication needs more testing, the authors explained. CAD systems for identifying lung nodules are available for radiologists' use to interpret chest CT imaging, but they are trained on adult data and whether they are effective in a pediatric population is unclear.
Hardie and colleagues conducted a study that compared the lung nodule detection performance of two CAD systems trained on adult data between low-dose (0.32 mSv) and standard-dose (1.77 mSv) pediatric chest CTs. The work included 73 patients (mean age, 14.7; age range, 4 to 20) who underwent both types of CT exams during the same encounter between November 2018 and August 2020; pediatric radiologists annotated nodules found on the scans to serve as the reference standard. The scans were processed using two lung-nodule CAD systems: FlyerScan and Medical Open Network for Artificial Intelligence (MONAI); the team evaluated these CAD systems' sensitivity for lesions between 3 mm and 30 mm.
The researchers reported the following:
| Performance of two CAD systems for detecting lung lesions in pediatric patients | ||
|---|---|---|
| Measure | FlyerScan | MONAI |
| Sensitivity | ||
| Standard dose CT | 76.9% | 67.6% |
| LDCT | 66.8% | 62.3% |
| Number of detected nodules | ||
| Standard dose CT | ||
| 3 mm | 33 | 16 |
| 4 mm | 46 | 39 |
| 5 mm | 38 | 32 |
| 6 mm | 27 | 24 |
| LDCT | ||
| 3 mm | 24 | 13 |
| 4 mm | 42 | 30 |
| 5 mm | 33 | 31 |
| 6 mm | 20 | 24 |
The group noted that for lesions equal to or larger than 7 mm, neither CAD system showed a consistent pattern of identification between standard and low-dose CT imaging.
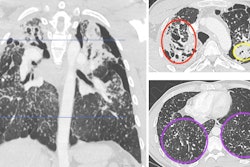
 12-year-old male patient who underwent chest CT due to hepatocellular carcinoma. Cropped axial CT images in pediatric patient showing CAD results operating at mean of two false positives per scan for both standard-dose and low-dose scans. Red contours represent FlyerScan CAD system detections. Cyan boxes represent MONAI CAD system detections. Blue "+" symbols represent annotated nodule center-of-mass coordinates, determining reference standard. (Left) Standard-dose image (1.39 mSv). Both CAD systems identified nodule. (Right) Low-dose image (0.34 mSv). Nodule was identified by FlyerScan but missed by MONAI. Images and caption courtesy of the AJR.
12-year-old male patient who underwent chest CT due to hepatocellular carcinoma. Cropped axial CT images in pediatric patient showing CAD results operating at mean of two false positives per scan for both standard-dose and low-dose scans. Red contours represent FlyerScan CAD system detections. Cyan boxes represent MONAI CAD system detections. Blue "+" symbols represent annotated nodule center-of-mass coordinates, determining reference standard. (Left) Standard-dose image (1.39 mSv). Both CAD systems identified nodule. (Right) Low-dose image (0.34 mSv). Nodule was identified by FlyerScan but missed by MONAI. Images and caption courtesy of the AJR.
Lower CAD system performance is likely due to differences in CT exam dose, the group explained, noting that "greater image noise associated with a lower dose may obscure subtle nodule characteristics that would otherwise help to distinguish the nodule from normal vasculature."
In any case, the study findings underscore a need for careful consideration when using LDCT with CAD systems to find small lung lesions in children, Hardie and colleagues concluded.
The complete study can be found here.