The timing and selection of which breast to image first matter when it comes to acquiring contrast-enhanced mammography (CEM) images, suggests research presented at the American Roentgen Ray Society (ARRS) annual meeting in Honolulu.
In a scientific online poster, a team led by Dr. Dennis Dwan from Beth Israel Deaconess Medical Center in Boston found that recombined images obtained earlier is significantly preferred in cancer lesion characterization, with a few instances showing that biopsy-proven lesions may appear more conspicuously on these images. It also found that breast imagers prefer craniocaudal over mediolateral oblique projection.
"Institutions should consider developing CEM protocols where the breast containing pathology is imaged first, around 2.5 minutes after contrast administration," Dwan and colleagues wrote.
CEM has been praised by researchers in previous research for having a similar diagnostic yield as MRI, as well as being more affordable and having fewer contraindications. Additionally, exams take about 10 minutes to perform. However, Dwan and colleagues noted that there is no consensus on best practices. This includes contrast dose or rate, as well as on the order of projection or laterality.
"There is also no discussion in the current literature on the optimal timing within this 10-minute timeframe," the researchers wrote. "If there is a suspicious or known malignancy, on one side, should that side be imaged first?"
Dwan and co-authors wanted to review basic background and protocol considerations for CEM and propose specific image acquisition protocol. It wanted to accomplish this by showing differences in cancer lesion characterization for images obtained at different time points during image acquisition.
The researchers collected data from 78 women with an average age of 58 years. They split the patient cohort into two groups of consecutive CEM cases. One included 40 cases between 2016 and 2018 that acquired craniocaudal views performed first. The other included 38 cases from 2019 and 2020 acquired with mediolateral oblique views performed first.
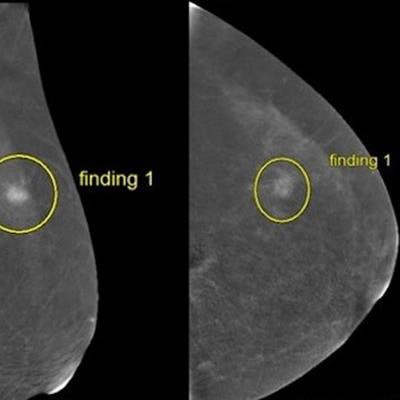
 An online scientific poster presentation led by Dr. Dennis Dwan from the Beth Israel Deaconess Medical Center found that projection order and acquisition time matter when it comes to contrast-enhanced mammography. These CEM images show an earlier-obtained image described as mass and a later-obtained image described as non-mass enhancement by the same reader for images of the same patient. Images courtesy of the ARRS.
An online scientific poster presentation led by Dr. Dennis Dwan from the Beth Israel Deaconess Medical Center found that projection order and acquisition time matter when it comes to contrast-enhanced mammography. These CEM images show an earlier-obtained image described as mass and a later-obtained image described as non-mass enhancement by the same reader for images of the same patient. Images courtesy of the ARRS.The side of pathology was at first imaged in either the craniocaudal or mediolateral oblique projection, also known as earlier-obtained imaging, followed by the contralateral side in the same projection. Then, imaging was repeated for the other projection, also known as later-obtained imaging.
From there, five readers evaluated cases for cancer visibility, confidence margin, and cancer conspicuity against background parenchymal enhancement (BPE). This made for a total of 390 instances reviewed.
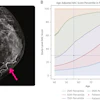
The researchers found that earlier-obtained images had an average acquisition time of 2.5 minutes, compared with 4.75 minutes seen for later-obtained images. In 35 of 390 instances (9%), an individual reader changed the reported lesion type between earlier and later imaging. Of the 35 instances, 28 reflected a situation where a finding was downgraded to a less conspicuous finding on later-obtained imaging.
The team also found that most readers preferred earlier-obtained images when evaluating the visibility of cancer, confidence in margins, and conspicuity of lesion against BPE (p < 0.001). Additionally, most readers preferred craniocaudal views over mediolateral oblique projection when assessing lesion conspicuity against BPE (p = 0.045). The researchers also reported no significant preference for evaluating lesion visibility (p = 0.078) or confidence in margins (p = 0.35).
The study authors suggested that further research exploring timing of CEM images may help increase exam specificity while maintaining sensitivity.