An ultrasound shear-wave elastography technique can effectively differentiate between metastatic and nonmetastatic cervical lymph nodes, according to preliminary research published in the March issue of the Journal of Ultrasound in Medicine.
In a retrospective study of 85 patients with superficial lymph-node lesions, investigators found that metastatic cervical lymph nodes had significantly higher shear-wave velocity values than nonmetastatic cervical lymph nodes. In addition, the shear-wave elastography technique neared 90% accuracy for differentiating between metastatic and nonmetastatic nodes, concluded the team led by Yingyan Zhao and Jiaying Xi of Changhai Hospital in Shanghai (J Ultrasound Med, March 2017, Vol. 36:3, pp. 557-563).
"Because of its noninvasive [nature], this technique applied to cancer patients has a broad prospect," Zhao told AuntMinnie.com.
An essential factor
The human body has 400 to 450 lymph nodes, of which about 60 to 70 are in the head and neck region. The presence or absence of regional lymph-node metastasis in cancer patients is an essential factor in disease staging, treatment, and prognosis, according to the authors.
"It is very important to detect and identify the nature of regional lymph nodes," Zhao said.
The researchers sought to assess the performance of Virtual Touch tissue imaging quantification (VTIQ) software (Siemens Healthineers) for the differential diagnosis of cervical lymph nodes. They retrospectively analyzed the conventional ultrasound and VTIQ images of 85 patients at Changhai Hospital from November to December 2015 who had superficial lymph-node lesions and a pathologically confirmed diagnosis.
Of the 85 nodes, 44 were metastatic and 41 were nonmetastatic. The nonmetastatic nodes included 24 cases of hematologic/lymphatic system disease and 17 reactive hyperplastic nodes.
The patients first received conventional 2D ultrasound exams using an Acuson S3000 ultrasound scanner (Siemens) and a 4- to 9-MHz transducer. Next, the lymph nodes' shear-wave velocity values were measured using the VTIQ software, which is based on acoustic radiation force impulse (ARFI) elastography. All studies were performed by a physician with extensive qualifications and experience in sonographic diagnosis, according to the researchers. Final pathologic diagnosis was later conducted on all nodes after either surgery or aspiration biopsy.
The metastatic lymph nodes had a mean shear-wave velocity of 4.29 ± 1.23 m/sec, while nonmetastatic nodes had a mean shear-wave velocity of 2.58 ± 0.50 m/sec. The difference was statistically significant (p < 0.001). The researchers generated a receiver operating characteristic (ROC) curve to determine the software's efficacy for the differential diagnosis of these lymph nodes.
| Performance of VTIQ software | |||||
| Differentiation | AUC, shear-wave velocity cutoff value | Accuracy | Sensitivity | Specificity | PPV, NPV |
| Metastatic vs. nonmetastatic lymph nodes | 0.953, 3.27 m/sec | 89.4% | 88.6% | 90.2% | 90.7%, 88.1% |
| Metastatic vs. hematologic/lymphatic system disease nodes | 0.943, 3.23 m/sec | 88.2% | 88.6% | 87.5% | 92.9%, 80.8% |
| Metastatic vs. reactive hyperplastic nodes | 0.968, 3.27 m/sec | 90.2% | 88.6% | 94.1% | 97.5%, 76.2% |
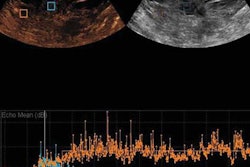
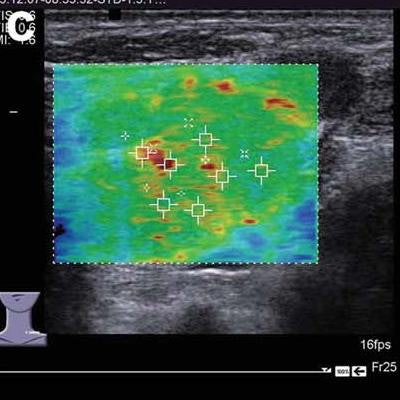
 Left: Images of metastatic cervical lymph node. (A) Irregular low-echo nodules can be seen on conventional ultrasound, but the structure of the lymph node hilum is unclear. (B) Using "quality mode" on the VTIQ software, the lesion appears green with some yellow, showing good elasticity. (C) Using "velocity mode" on the VTIQ software, the shear-wave velocity values are shown for different points in the lesion. Right: Images of nonmetastatic lymph node. (A) An oval hypoechoic nodule can be seen on the conventional ultrasound, but the structure of the lymph node hilum is also unclear. (B) and (C), same descriptions as for previous image. All images courtesy of the Journal of Ultrasound in Medicine.
Left: Images of metastatic cervical lymph node. (A) Irregular low-echo nodules can be seen on conventional ultrasound, but the structure of the lymph node hilum is unclear. (B) Using "quality mode" on the VTIQ software, the lesion appears green with some yellow, showing good elasticity. (C) Using "velocity mode" on the VTIQ software, the shear-wave velocity values are shown for different points in the lesion. Right: Images of nonmetastatic lymph node. (A) An oval hypoechoic nodule can be seen on the conventional ultrasound, but the structure of the lymph node hilum is also unclear. (B) and (C), same descriptions as for previous image. All images courtesy of the Journal of Ultrasound in Medicine.False negatives
There were five false negatives for metastatic nodes.
"The possible reason is that in the early stage of lymph-node metastasis, the tumor cells only invade into the cortex of nodes, while most tissues remain unaffected, with no notable change in hardness," the authors wrote. "Alternatively, it is possible that in the late stage, tumor cell invasion causes liquefaction of whole lymph nodes, leading to tissue softening and decreased [shear-wave velocity] values."
Three false-positive results were found in the hematologic/lymphatic disease nodes. These may have been due to increased hardness caused by the adhesion and fusion of enlarged lymph nodes, according to the group.
"Further study is required to assess the changes in [shear-wave velocity] values of enlarged lymph nodes in hematologic/lymphatic system diseases at different stages," they wrote.
Only one case of reactive hyperplastic nodes produced a false-positive result; the increased lesion hardness may have been caused by internal lesions becoming organized due to a long-term presence, the authors speculated.
Helping clinical diagnosis
Metastatic and nonmetastatic lymph nodes present differently on shear-wave elastography, the authors concluded.
"Thus, the VTIQ technology with [shear-wave velocity] measurement could provide evidence for differential diagnosis and help clinical diagnosis," they wrote. "However, a few metastatic lymph nodes showed false-negative results, with low [shear-wave velocity] values and relatively softer tissues. Therefore, the value of VTIQ in differentiating metastatic and nonmetastatic cervical lymph nodes still needs further exploration with large-sample studies."
The researchers acknowledged a number of limitations of their work, including a relatively small sample size and its inclusion of relatively few types of disease.
"Moreover, those causes have not yet been thoroughly studied in metastatic lymph nodes with different courses, hematologic/lymphatic system disease, and hardness changes at different stages," they wrote. "Therefore, further studies are warranted for those purposes."