MIAMI BEACH, FL - FDG dose can be reduced by 50% in PET scans without adversely affecting diagnostic performance, even with shorter acquisition times, according to a study presented this week at the Society of Nuclear Medicine (SNM) annual meeting.
Researchers from the University of Washington (UW) in Seattle evaluated image quality at three points along an acquisition timeline, and while they found some image degradation, the decline was not enough to make any images unacceptable.
No standard FDG dose
Although previous research has investigated FDG dose and whether clinicians can scan faster with good results, debate continues about the optimal imaging protocol.
"There is simply no standardization on FDG dose and no definitive answer on what is the right amount to inject," said lead study author Adam Alessio, PhD, a research assistant professor in UW's department of radiology. "Some places inject 15 [mCi] and some places inject 5 [mCi], and life goes on."
In addition, despite advances in PET instrumentation and image reconstruction over the past 10 years, UW researchers asserted that few studies have evaluated whether administered FDG dose can be reduced in current imaging systems without a loss in overall diagnostic utility.
"Certainly, there are concerns around the risks of radiation, so this is also a motivation," Alessio added. "Also, if a facility has limited resources and wants to save money, it could get by with less dose and save on costs."
In the study, 20 patients with a mean weight of 165 lb (range, 105-297) received whole-body PET/CT scans (Gemini TF, Philips Healthcare) one hour after injection of 10 mCi of the radiopharmaceutical. Fixed image acquisition durations were set at four minutes, two minutes, and one minute per field-of-view (FOV).
Two reviewers evaluated 115 lesion sites to determine PET/CT's accuracy, with the full duration of four minutes used as the reference standard. Maximum standardized uptake values (SUVs) of primary lesions and noise in the liver were evaluated, along with image quality, which was rated on a scale of 1 (unacceptable) to 5 (excellent).
"We wanted to evaluate detection accuracy, so we had the reviewers go through all the lesion cycles to see if the accuracy degrades as we go to lower duration studies," Alessio explained.
The analysis found that the one-minute and two-minute scans did not change staging in any patient, compared with the full-duration scan. The two-minute study had identical specificity to the full-duration scan and four false-negative results in two patients, who had a total of more than seven lesions. Sensitivity was 98%, with a specificity of 100%.
The one-minute study failed to detect lesions in 12 patients, compared with the full-duration scan. In total, it produced nine false positives and nine false negatives. Sensitivity was 91% and specificity was 93%.
 |
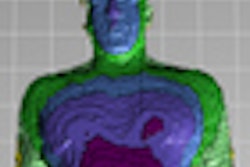
| The series of images shows image quality over the course of the PET/CT scan in a 178-lb patient. All images courtesy of Adam Alessio, PhD. |
 |
Regarding image quality, the full four-minute study achieved the best image quality, which the two readers rated an average of 4.25. As image acquisition time decreased, so did image quality. Readers rated images from the two-minute duration as 3.8 and from the one-minute duration as 2.9.
"The full-duration studies were deemed to be good to excellent [image] quality; the half-duration were good to very good quality, and the quarter-duration was a little worse," Alessio said. "None of the studies -- even the quarter-duration -- were considered unacceptable. They all had information content and were within the bounds of our two readers for acceptability."
 |
| In these images of a 125-lb patient, the half- and full-duration studies had the same findings, whereas there was a false negative in the upper right lung on the quarter-duration scan. |
 |
Noise increased 23% at two minutes and 58% for the one-minute study, as measured in a uniform region of the liver, compared with images from the four-minute acquisition time.
Maximum SUVs of primary lesions changed just 1% (± 1%) for the two-minute duration and 3% (± 2%) for the one-minute scan.
"The conclusion you could draw from this data is that a reduction in acquisition duration led to smaller reductions in performance, but no changes in the staging of patients," Alessio said. "All full-duration studies were considered good to excellent, and reductions down to a quarter duration did not cause any clinical changes in quantitation."
Alessio cited limitations to the research, such as the small patient sample and the fact that there was no gold standard to compare results, only the four-minute duration as a reference standard.
He also cautioned SNM attendees to be careful how they interpret the results; they should not walk away from the presentation thinking that reducing dose by 50% should be the standard imaging protocol. "We are not always trying to lower our dose," he said. "There could be people in this room who need to increase their dose to get the quality necessary for FDG imaging."
"There is more to the story than just what you inject; it is how you scan the patient," he said, regarding fluctuations in dose optimization. "This talk is about protocol refinement. Just because you have always injected 10 mCi, it doesn't mean you continue to inject 10 mCi. There may be a time when you need to be rational about the dosage you inject."