Radiology departments have been working overtime since the outbreak of COVID-19. But how nuclear medicine can contribute to the healthcare of the world's populations remains somewhat unclear, according to an article published online April 7 in Nuklearmedizin.
To help shed some light on what superficially might seemed like a limited role for nuclear medicine, a group of researchers at the University Hospital Bonn in Germany have proposed several clinical situations in which nuclear medicine can be beneficial, even in a tangential way.
"One of the hallmarks of a critical course of COVID-19 is the development of severe acute respiratory distress syndrome," wrote Dr. Susanne Lütje and colleagues from the department of nuclear medicine and Clinic for Diagnostic and Interventional Radiology. "As management of COVID-19 can be considered a multidisciplinary approach involving various medical specialties, we here review the first FDG-PET/CT scans of COVID-19 to discuss how nuclear medicine could contribute to management of this disease."
COVID-19 is caused by infection with the SARS-CoV-2 virus, which can remain asymptomatic for days before it leads to fever, cough, respiratory issues, and fatigue. Many patients progress to pneumonia and acute respiratory distress syndrome (ARDS), with an estimated 5% of patients becoming critically ill with severe lung ailments.
To diagnose and evaluate these conditions, CT is one of the first options, given its ability to detect ground-glass opacities in the lungs. In addition, FDG-PET has long been used to detect and evaluate the severity of inflammation relative to lung diseases, monitor its progression, and determine the efficacy of follow-up treatment.
Lütje and colleagues suggest that FDG-PET/CT be used to monitor response to respiratory therapy and help determine a patient's recovery time. They cited a May 2020 study by Qin et al in which researchers from China found a trend among four COVID-19 patients where greater FDG uptake in SARS-CoV-2-induced pulmonary lesions correlated with longer recuperative times. A maximum standardized uptake value (SUVmax) of 4.6 was observed in one patient who recovered approximately 17 days after the onset of symptoms, while another patient with a SUVmax of 12.2 took more than 26 days after first symptoms to return to health (EJNMMI, May 2020, Vol. 47:5, pp. 1281-1286).
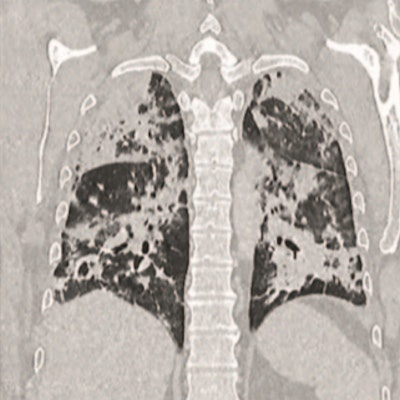
 CT images of two patients with COVID-19 pulmonary manifestations. Incidental finding of SARS-CoV-2 infection in an asymptomatic 60-year old female (A) show peripheral ground-glass opacities in basal segments of the right lung. A polymerase chain reaction test confirmed SARS-CoV-2 infection on molecular level. A 51-year-old SARS-CoV-2-positive male (B) with pronounced bilateral pulmonary involvement of COVID-19 was hospitalized in an intensive care unit. Typical lesion spread to the center of the lungs and consolidation is present. Images courtesy of Nuklearmedizin.
CT images of two patients with COVID-19 pulmonary manifestations. Incidental finding of SARS-CoV-2 infection in an asymptomatic 60-year old female (A) show peripheral ground-glass opacities in basal segments of the right lung. A polymerase chain reaction test confirmed SARS-CoV-2 infection on molecular level. A 51-year-old SARS-CoV-2-positive male (B) with pronounced bilateral pulmonary involvement of COVID-19 was hospitalized in an intensive care unit. Typical lesion spread to the center of the lungs and consolidation is present. Images courtesy of Nuklearmedizin.FDG uptake patterns in other parts of a patient's body also can be attributed to COVID-19, which is known to damage the heart, kidneys, or bone marrow. Hence, whole-body PET could be used as a "noninvasive readout to assess [chronic] and concomitant organ damage," the authors wrote, citing a March 2020 report by Zou et al, which found FDG uptake in the bone marrow of one COVID-19 patient (Radiology, March 6, 2020).
"Taken together, although FDG-PET/CT may not be routinely used in COVID-19 management, especially not in an emergency setting, first data indicate that this imaging modality could play a complementary role in COVID-19 management," Lütje and colleagues concluded. "FDG-PET/CT may reflect changes in FDG-avidity in pulmonary lesions as well as in other organs during the course of COVID-19, potentially clarifying differential diagnosis, estimating the extent of organ involvement and characterizing treatment response during follow-up."




COVID-19_FDG_PET_CT_JNM_Albano_Image_G_400.png?auto=format%2Ccompress&fit=crop&h=167&q=70&w=250)













