Coronary CT angiography (CCTA) shows promise for helping clinicians determine whether a patient requires invasive coronary angiography -- as well as for planning strategies for managing interventions to treat their disease, according to a review published January 6 in Radiology: Cardiothoracic Imaging.
CCTA could improve how heart disease patients are managed, wrote a team led by Dr. Georgios Tzimas of the University of British Columbia in Vancouver.
"Integration of CCTA in the procedural planning of patients considered for invasive evaluation could potentially facilitate the course of invasive coronary angiography, enhance diagnostic and therapeutic intervention, and improve clinical outcomes," the group noted,
CCTA is proving to be an effective, noninvasive way to assess the presence, extent, and severity of coronary artery disease (CAD) in patients with stable angina, in part due to advances in scanner hardware and software that generate more useful clinical information from a single study, the team noted.
"Beyond merely identifying the presence of CAD and assessing stenosis severity, CCTA now allows for the identification and characterization of plaques, lesion length, and fluoroscopic angle optimization, as well as enables the assessment of the physiologic extent of stenosis through CT-derived fractional flow reserve, and may even allow for the prediction of the response to revascularization," Tzimas and colleagues wrote.
These expanded capabilities suggest that CCTA could help clinicians better determine whether a patient needs invasive coronary angiography and better plan disease intervention, according to the investigators.
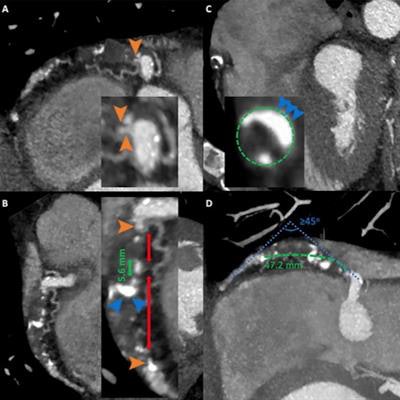
 Images from coronary CT angiography for chronic total occlusion (CTO) in a 55-year-old man who presented with chest pain. (A-C): Oblique reformatted CT images show an occlusion in the proximal to mid with segment of right coronary artery. Long-segment CTO (green dashed line) measuring 47.2 mm tapered tip stump (orange arrowheads) and mild tortuosity. Calcification (blue arrowheads) involving less than 50% of the vessel cross-sectional area within the occlusion site (green dashed circle). Presence of two complete interruptions (double red arrows) of the contrast opacification separated by contrast-enhanced segment of greater than 5 mm (double green arrow). (D) Maximum intensity projection image shows presence of bending of greater than 45 degrees within the occlusion route (blue dotted lines). Green dashed line indicates coronary course. Images and caption courtesy of the RSNA.
Images from coronary CT angiography for chronic total occlusion (CTO) in a 55-year-old man who presented with chest pain. (A-C): Oblique reformatted CT images show an occlusion in the proximal to mid with segment of right coronary artery. Long-segment CTO (green dashed line) measuring 47.2 mm tapered tip stump (orange arrowheads) and mild tortuosity. Calcification (blue arrowheads) involving less than 50% of the vessel cross-sectional area within the occlusion site (green dashed circle). Presence of two complete interruptions (double red arrows) of the contrast opacification separated by contrast-enhanced segment of greater than 5 mm (double green arrow). (D) Maximum intensity projection image shows presence of bending of greater than 45 degrees within the occlusion route (blue dotted lines). Green dashed line indicates coronary course. Images and caption courtesy of the RSNA.In their review, Tzimas's team outlined a few ways the technology could improve patient care and outcomes:
- CCTA could be used to craft an "anatomy roadmap" for physicians performing interventional procedures. "The ability of CCTA to accurately measure lesion length may be employed in prior planning for percutaneous coronary interventions, as it allows a complete visualization of coronary vasculature without foreshortening and overlapping, which is frequently encountered with invasive angiography," the group wrote.
- CCTA could be used to quantify and characterize heart plaque. "The ability of CCTA not only to identify and quantitatively evaluate structure of atherosclerotic plaque but also provide detailed anatomic information of the entire coronary vasculature makes it a powerful diagnostic tool in preprocedural planning and periprocedural guidance of chronic total occlusion percutaneous coronary interventions," the researchers wrote.
- CCTA could go beyond anatomic classifications of coronary lesions to "evaluation of coronary translesional physiology," according to Tzimas and colleagues.
CCTA's capacity for cardiac indications beyond diagnosis invites further research, the authors concluded.
"The opportunity to use CCTA technologies and advanced analytics is enabling the transition of CCTA from strictly being used for diagnosis to a tool that can be used to plan coronary interventions," they wrote. "The potential of CCTA needs to be further explored in prospective trials to evaluate to what extent this modality may enable more efficient catheterization laboratory use, more complete revascularization, and improved clinical outcomes."