Mounting evidence suggests that coronary CT angiography (CCTA) may be the best first-line test for evaluating possible coronary artery disease (CAD). Physicians from Virginia and Texas detailed five features of CCTA that support this idea in an article published online August 28 in the Journal of Thoracic Imaging.
The group, led by first author Dr. Christopher Maroules from the Naval Medical Center in Portsmouth, VA, reviewed current research centered on the use of CCTA for patients with chest pain who are suspected of having coronary artery disease. They found that CCTA was well-positioned to be a first-line test for a variety of reasons, including those described below.
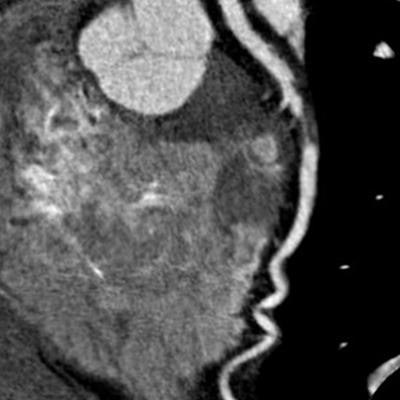
 CCTA scan indicates severe stenosis in the left anterior descending artery of a 52-year-old patient with stable chest pain. Image courtesy of Dr. Christopher Maroules.
CCTA scan indicates severe stenosis in the left anterior descending artery of a 52-year-old patient with stable chest pain. Image courtesy of Dr. Christopher Maroules.1. Effective gatekeeping for cardiac catheterization
In addition to CCTA being the only noninvasive imaging modality that provides a reliable depiction of the coronary arteries, numerous large-scale trials have demonstrated the test's capacity to improve the diagnosis of obstructive CAD as well, Maroules and colleagues noted.
What's more, combining noninvasive functional tests such as CT myocardial perfusion and CT fractional flow reserve with CCTA provides clinicians with more information concerning coronary stenosis. Ultimately, these benefits may enable CCTA to detect pathology and prevent unnecessary invasive procedures more efficiently than other methods.
2. Utility for guiding revascularization and therapeutic decision-making
Recent studies, such as the Prospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE) and the Scottish Computed Tomography of the Heart (SCOT-HEART) trial, have suggested that CCTA may be better than standard clinical evaluation at discerning which patients require revascularization versus medical therapy -- particularly due to its high diagnostic yield for obstructive CAD.
3. Advanced risk stratification
CCTA has the ability to assess the full spectrum of coronary plaque and use this information to stratify a patient's risk of heart disease and cardiac events. On the other hand, stress electrocardiography, stress imaging, and other conventional functional tests are limited to identifying only patients with advanced stenosis.
4. Improvement in patient outcomes
In a meta-analysis of randomized controlled trials comparing CCTA with functional testing, Bittencourt et al reported that CCTA reduced the relative risk of heart attack in patients presenting with chest pain by 31%. A recent follow-up study of the SCOT-HEART trial also found that CCTA reduced the risk of either heart attack or death by approximately 50%.
A potential caveat of these improved outcomes, however, is a greater financial burden: CCTA cost an average of $254 more than functional testing in PROMISE and $462 more than the standard of care in the SCOT-HEART trial.
5. Support from various society guidelines
Several societies have endorsed the use of CCTA as an effective diagnostic test for evaluating stable chest pain in patients suspected of having CAD. Notably, the U.K. National Institute for Health and Care Excellence (NICE) 2016 clinical guideline recommends CCTA as a first-line test.
"Given the expansion of CT technologies to include functional strategies for evaluating ischemia both with and without vasodilators, CCTA is poised to become the comprehensive examination for stable chest pain and anginal equivalent cardiopulmonary symptoms," the authors wrote.

















