Radiopharmaceutical producer and distributor P.E.T.Net Pharmaceuticals has opened four new facilities in the southeastern U.S. The new sites are in Columbia, SC; Jacksonville, FL; Raleigh-Durham, NC; and Winston-Salem, NC. Knoxville, TN-based P.E.T.Net now has 28 cyclotron-equipped radiopharmacies nationwide.
By AuntMinnie.com staff writersNovember 15, 2001
Related Reading
P.E.T. Net to operate Wake Forest FDG facility, November 1, 2001
P.E.T.Net licenses beta-amyloid plaque-labeling technology, October 10, 2001
P.E.T.Net adds radiopharmacies, August 2, 2001
P.E.T.Net opens research facility with UCLA, July 4, 2001P.E.T.Net Pharmaceuticals taps Hiatt for VP post , May 9, 2001
Copyright © 2001 AuntMinnie.com
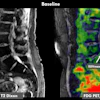














![A 53-year-old patient (patient number four) with a recurrent pituitary adenoma with extension of a cystic component of disease to the medial temporal lobe apparent on MRI (contoured in blue), and extension of disease to the left sphenoid bone and orbital apex apparent on [68Ga]Ga-DOTA-TATE (contoured in yellow).](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/04/pituitary-tumor.QGsEnyB4bU.jpg?auto=format%2Ccompress&dpr=2&fit=crop&h=167&q=70&w=250)

